The mDOT Center
Transforming health and wellness via temporally-precise mHealth interventions






mDOT@MD2K.org
901.678.1526
901.678.1526


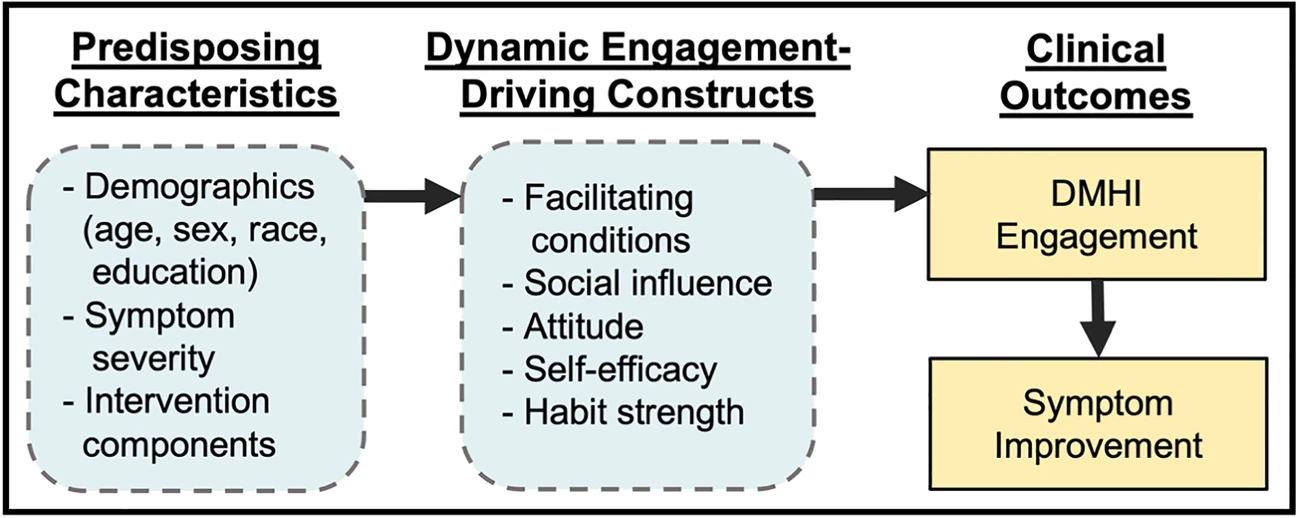
Depression and anxiety are highly comorbid and costly diseases. Evidence-based psychotherapy is the first-line treatment, but is underutilized and not scalable. Digital mental health interventions (DMHIs), delivered via the internet and/or mobile apps, have evolved as efficacious and potentially scalable treatments. To date, however, effectiveness in routine care is limited by insufficient patient engagement. In order to achieve the transformative potential of DMHIs, we must identify strategies to keep patients engaged without adding human support in a form that would limit scalability. Automated motivational push messaging (AMM) and light-touch human coach support (CS) offer two such strategies. The proposed research tests these strategies, while drawing preliminary conclusions about a hypothesized model of DMHI engagement based on the technology adoption and treatment adherence literature. I will recruit N=76 primary care patients with depression and/or anxiety via provider referral to an 8-week 2×2 factorial clinical trial whereby participants will all receive access to a DMHI with known efficacy and be randomized to an engagement strategy condition (i.e., a previously-validated CS protocol, newly-developed AMM, both or neither). To further understand how AMMs function, message delivery in the AMM arms will be micro-randomized: each day participants will be randomized to receive a message or not, such that they receive an average of 4.2 messages/week. Micro-randomization allows causal inference about the near-term impact of message delivery (i.e., are AMMs a cue to action) and the relationship between message impact and context (e.g., time of day the message is delivered). Measured outcome data will comprise level of engagement (operationalized as minutes of DMHI use), weekly self-reports on hypothesized engagement-driving constructs, and weekly self-reports of clinical outcomes. I will test the impact of each strategy on measured outcome data (Aim 2) and explore relationships between hypothesized engagement-driving constructs and DMHI engagement (Aim 3). Clinical outcomes will be assessed, however, consistent with the experimental therapeutics model, this research leverages a DMHI with known efficacy, allowing the focus to be an upstream target (patient engagement) rather than the clinical outcomes themselves. The overarching goal is to influence the target so as to ultimately enhance clinical effectiveness.
This SP is interested in the personalization algorithms proposed by TR&D2, in particular, the use of these stochastic algorithms to determine the randomization probabilities in the MRT. Further this SP is very interested in using the (under development) pJITAI toolbox. If the TR&D algorithms under Aims 1 and 2 are demonstrated to be robust, SP would be potentially interested in including extra participants so to conduct a feasibility study for use in informing SP’s future research.
Mental Health, SP, TR&D2
You must be logged in to post a comment.
No Comments