The mDOT Center
Transforming health and wellness via temporally-precise mHealth interventions






mDOT@MD2K.org
901.678.1526
901.678.1526


Tobacco use is the leading cause of death and disability in the United States, and is associated with at least 16 different types of cancers. Though nationwide rates have declined, tobacco use has become concentrated in populations that have been historically marginalized and plays a critical role in health inequities, accounting for 34% of the socioeconomic gradient in all-cause mortality and 62% in smoking related diseases, including cancers of the lip/oral cavity/pharynx, esophagus, larynx, trachea, and lung. These populations also experience adverse Social Determinants of Health (SDOH), which frequently co-occur with tobacco use, and contribute to limited access and engagement with evidenced-based interventions (EBIs) for tobacco cessation. Consequently, addressing SDOH and tobacco use concurrently may address barriers to engaging in EBIs for tobacco cessation and ultimately reduce the impact of tobacco use among individuals living in poverty. However, the effectiveness and cost effectiveness of strategies to concurrently increase the reach of EBIs for tobacco cessation and mitigate the effects of SDOH among individuals living in persistent poverty areas is unknown.
CP16 is highly significant for the mDOT Center because it addresses tobacco use, the leading cause of preventable death and disability in the United States, which disproportionately affects populations living in persistent poverty. By focusing on health inequities and adverse social determinants of health (SDOH), CP16 provides the Center with an opportunity to demonstrate how advanced digital health tools can be applied in underserved populations where traditional interventions often fail to gain traction. The project allows the mDOT Center to test its computational, sensing, and adaptive intervention technologies in real-world community health settings, ensuring that the Center’s innovations are not only scientifically rigorous but also equitable and scalable. In doing so, CP16 reinforces the Center’s mission of bridging the gap between technical development and impactful health outcomes.
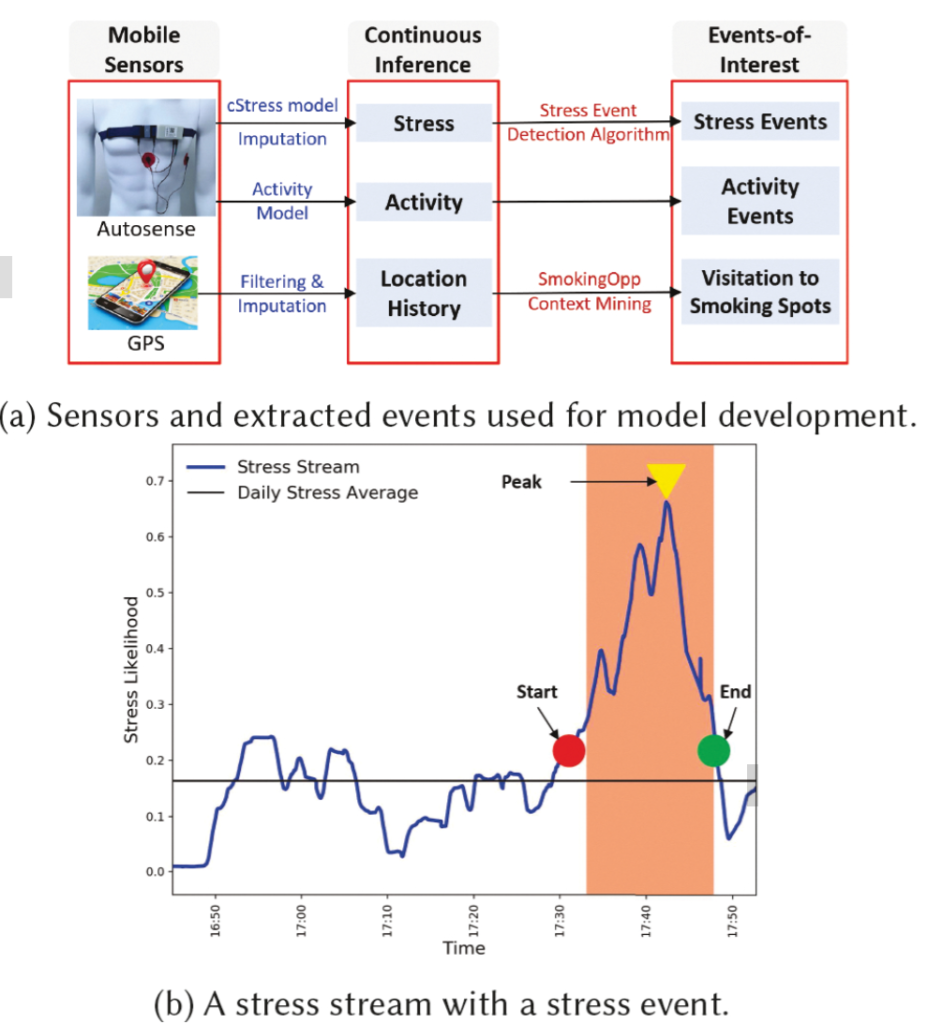
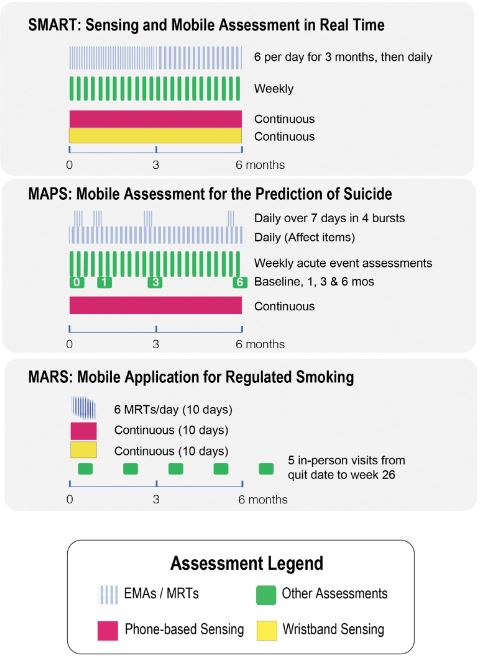
CP16 leverages the mDOT Center’s expertise in multimodal sensing, machine learning, and adaptive intervention design to enhance the reach and effectiveness of evidence-based interventions in populations living in persistent poverty. The project integrates TR&D3’s wearable sensing technologies and micromarker computation with TR&D1’s machine learning models for stressor detection and digital phenotyping. These tools are embedded into HC2’s community-based framework, which engages community health centers, Cooperative Extension Systems, and American Indian organizations. Data from wearables and smartphones are used to capture real-time information on stress, craving, activity, and engagement, which informs adaptive delivery of tobacco cessation and obesity prevention strategies. Through continuous feedback between community stakeholders, computational teams, and implementation scientists, CP16 develops culturally tailored, context-aware, and equitable digital health solutions that address both behavioral risks and social determinants of health in underserved populations.
The relationship between CP16 and TR&D3 operates as a dynamic push/pull exchange that ensures innovations are both technologically advanced and contextually relevant. TR&D3 pushes novel sensing technologies, optimized wearables, and multimodal micromarker computation into CP16, equipping the project with tools to monitor stress, craving, and health behavior patterns in naturalistic environments. CP16, in turn, pulls from TR&D3 by defining the applied needs of populations living in persistent poverty—emphasizing usability, cultural sensitivity, privacy, and scalability in community health contexts. This ongoing feedback loop allows TR&D3’s technologies to be stress-tested and refined in diverse, real-world settings, while CP16 gains access to state-of-the-art sensing and analytic capacity that strengthens its intervention strategies.
The collaboration with TR&D3 directly impacts CP16 by improving the quality, precision, and contextual relevance of its interventions. By leveraging TR&D3’s sensing systems and computational methods, CP16 is able to generate more accurate and continuous measures of behavioral risk factors, stressors, and intervention engagement among populations in persistent poverty. These advances enable the tailoring of evidence-based interventions in real time, supporting both tobacco cessation and obesity prevention efforts in culturally diverse communities. The integration of TR&D3 innovations ensures that CP16 not only evaluates the effectiveness of these interventions but also enhances their scalability and sustainability. As a result, CP16 is positioned to make a meaningful contribution to reducing health disparities, while simultaneously providing the mDOT Center with critical insights into how its technologies perform in high-need, underserved populations.
CP, Emotional Context, Smoking Cessation, Stress, TR&D1
You must be logged in to post a comment.
No Comments